
Blog
Carotid Artery Disease: Symptoms & Treatment Options
Roughly 80 percent of strokes are preventable, yet carotid artery disease often gives no warning before a stroke strikes. That statistic alone should change how


Arthritis affects over 54 million adults in the United States, and for many patients in South Florida, the pain and stiffness can be relentless enough to disrupt daily life, sleep, and independence.
At South Florida Multispecialty Medical Group, we see this reality every day in our rheumatology practice. As a board-certified rheumatologist, I work with patients ranging from active 40-year-olds with early-onset osteoarthritis to older adults managing severe rheumatoid arthritis across multiple joints. Over the years, one question keeps coming up more than almost any other: “Doctor, is stem cell therapy right for me?”
It’s a fair question and an important one. Stem cell therapy sits at the intersection of genuine scientific innovation and considerable hype. This article offers an honest, clinically grounded look at what stem cell therapy is, how it works for arthritis specifically, who makes a good candidate, and what you can realistically expect from treatment here in Miami.
Stem cell therapy is a form of regenerative medicine that uses the body’s own repair mechanisms to address tissue damage and chronic inflammation rather than masking symptoms with medication alone. At its core, stem cells are unspecialized cells with two remarkable abilities: they can renew themselves and differentiate into specialized cell types such as cartilage cells, bone cells, or muscle cells.
For arthritis patients, this matters enormously. Arthritis, whether osteoarthritis, rheumatoid arthritis, or psoriatic arthritis, is fundamentally a disease of tissue breakdown and chronic inflammation. Conventional treatments like NSAIDs, DMARDs, and corticosteroid injections manage symptoms effectively, but they do not regenerate damaged cartilage or reverse joint degeneration. Stem cell therapy aims to do something more ambitious: promote tissue repair from within.
The science behind this is evolving rapidly. Evidence from preclinical and clinical studies suggests that mesenchymal stem cell (MSC) therapy can reduce inflammation, modulate immune responses, and promote tissue repair in arthritic joints. (PubMed/NIH, 2025) We are not talking about a silver bullet, but we are talking about a treatment approach with meaningful potential for the right patients.
Not all stem cells are the same, and the type used matters significantly for safety, legality, and clinical outcomes. In our hospital at SFL Medical Group, we focus on approaches that meet FDA guidelines and offer the strongest evidence base.

MSCs are the most widely used cell type in arthritis treatment research. They are harvested from bone marrow (known as Bone Marrow Aspirate Concentrate or BMAC) or adipose (fat) tissue. MSCs have strong anti-inflammatory and immunomodulatory properties, which makes them particularly relevant for conditions like rheumatoid arthritis and psoriatic arthritis, where immune dysregulation drives joint destruction. We now routinely evaluate patients for MSC-based therapies as part of our regenerative medicine program.
BMAC is collected directly from the patient’s own iliac crest (the pelvic bone) through a minimally invasive aspiration procedure. Because the cells come from the patient, they carry a very low risk of immune rejection. BMAC is one of the few regenerative approaches that is legally and ethically sound under current FDA guidelines, provided it is used with minimal manipulation. For moderate arthritis, BMAC-based stem cell therapy can provide relief lasting two to five years or more for some patients.
Patients often ask us about umbilical cord stem cell injections they have seen marketed online. I always give the same candid answer: under current FDA regulations, allogeneic (donor-derived) stem cells including umbilical cord tissue are not approved for arthritis treatment in the United States. Clinics offering these procedures are operating outside FDA-approved indications. We prioritize your safety above all else, which is why we only recommend approaches supported by credible evidence and aligned with federal regulatory standards.
Understanding the mechanism helps patients make informed decisions. Here is how a stem cell therapy in Miami protocol for arthritis typically unfolds in our practice:
Before we recommend anything, we conduct a thorough evaluation. This includes a review of imaging (X-rays, MRI), blood markers for inflammation (CRP, ESR, RF, anti-CCP), a physical examination of the affected joints, and a detailed discussion of your symptoms, treatment history, and lifestyle goals. We never rush this step. In our experience, the patients who do best with regenerative therapies are those who are properly screened and have realistic expectations going in.
For BMAC-based treatment, we perform a minimally invasive bone marrow aspiration under local anesthesia. This typically takes under 30 minutes. For adipose-derived MSCs, a small amount of fat is collected through a micro-liposuction technique. Both procedures are performed right here in our Miami facility.

Once collected, the aspirate is placed in a centrifuge that spins at high speed to separate and concentrate the stem cells and growth factors. This concentrated preparation is what gets injected into the affected joint. The entire process from collection to injection can take as little as one to two hours.
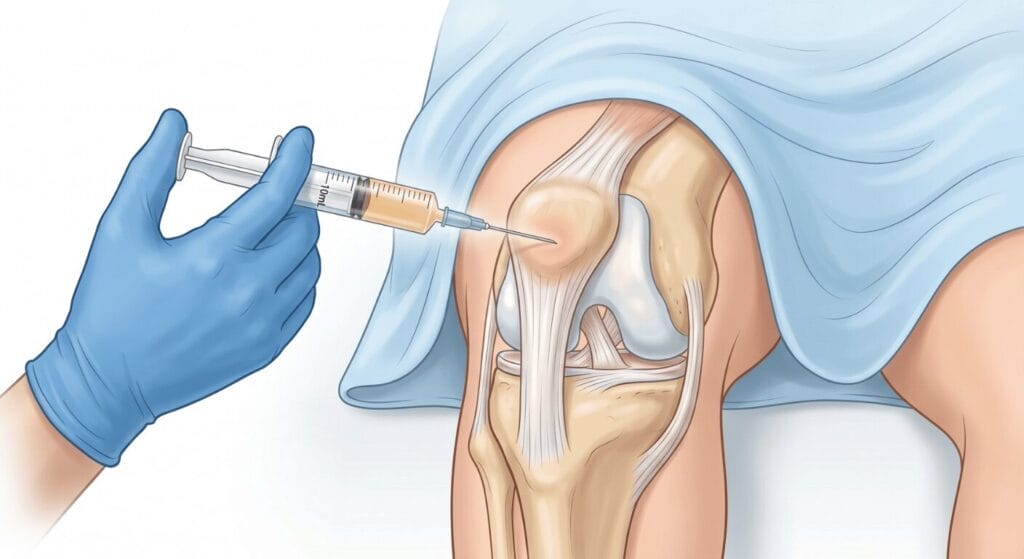
Accuracy matters enormously in joint injections. We use ultrasound or fluoroscopic guidance to deliver the stem cell preparation precisely into the target joint space, whether that is the knee, hip, shoulder, ankle, or another affected area. Patients tell me this feels far less intimidating than they expected, and most are back home the same day.
After the injection, we recommend a structured recovery plan. This typically involves a brief period of modified activity, followed by physical therapy to support joint rehabilitation and maximize the regenerative benefit. We schedule follow-up appointments to monitor progress at four weeks, eight weeks, and six months post-treatment.

One of the most significant and perhaps underappreciated mechanisms of MSC therapy is immunomodulation rather than simple regeneration. In rheumatoid arthritis and other inflammatory arthritides, the immune system is the aggressor. T-cells, macrophages, and pro-inflammatory cytokines like TNF-alpha and IL-6 drive joint inflammation and cartilage erosion.
MSCs intervene in this process by secreting anti-inflammatory signals, suppressing overactive immune cells, and promoting a more healing-oriented local environment in the joint. Clinical trials including the REMODEL and REMEDY studies have demonstrated improved outcomes in patients receiving MSC-based interventions for autoimmune and inflammatory joint conditions. This is why, in our rheumatology practice, we see MSC therapy as a potentially powerful adjunct for patients with inflammatory arthritis who are not achieving adequate control with biologics or DMARDs alone.
For osteoarthritis, the mechanism shifts somewhat toward cartilage support. MSCs can stimulate chondrocyte activity and release growth factors that slow cartilage breakdown and reduce the pain signaling associated with degenerative joint changes. Pairing regenerative treatment with an anti-inflammatory diet can further support joint healing. Most patients start noticing improvement in pain, stiffness, and joint function within four to twelve weeks after stem cell injections, with continued improvement possible for up to one to two years.
This is the question I get most often, and the honest answer is: not everyone. Stem cell therapy is not a replacement for all arthritis treatments, and candidacy requires careful clinical evaluation. If you are unsure whether your joint pain warrants specialist attention, our guide on when to see a rheumatologist is a helpful starting point. Here is what we look for:
Patients who tend to respond best to stem cell therapy for arthritis generally share these characteristics:
We tell patients honestly when stem cell therapy is unlikely to help or could be contraindicated. These situations include:
Age alone does not disqualify a patient. We have treated patients in their 70s who were excellent candidates and younger patients in their 40s who were not. What matters most is the extent of joint damage, overall health status, and the specific type and stage of arthritis. During your consultation at SFL Medical Group, we build a complete picture before making any recommendation.
Patients frequently ask how stem cell therapy stacks up against other options. Here is a practical comparison based on what we use in clinical practice:
| Treatment | Mechanism | Duration of Effect | Invasiveness | Best For |
|---|---|---|---|---|
| NSAIDs / Oral Medications | Symptom control, anti-inflammatory | Days to weeks | Non-invasive | Mild to moderate flares |
| Corticosteroid Injections | Reduces inflammation rapidly | Weeks to months | Minimally invasive | Acute flare-ups, short-term relief |
| PRP Therapy | Growth factors stimulate healing | 6 to 18 months | Minimally invasive | Mild to moderate OA, tendinopathy |
| Stem Cell Therapy (BMAC) | Regeneration + immunomodulation | 2 to 5+ years | Minimally invasive | Moderate OA, inflammatory arthritis |
| Biologic DMARDs | Immune system modulation | Long-term with continued dosing | Injections or infusions | Rheumatoid, psoriatic arthritis |
| Joint Replacement Surgery | Replaces damaged joint entirely | 15 to 20+ years | Major surgery | Severe, end-stage arthritis |
Stem cell therapy sits in an important middle ground. It offers meaningfully longer relief than PRP or cortisone injections and avoids the recovery and risks associated with joint replacement surgery, making it a compelling option for patients who are not ready or not appropriate for surgical intervention. For patients dealing specifically with knee pain treatment, this approach has shown particularly meaningful results in our practice.
We believe in full transparency with every patient who walks through our doors. Stem cell therapy for arthritis carries real limitations and deserves honest discussion, not sales-style enthusiasm.
From a regulatory standpoint, the FDA currently approves stem cell therapies primarily for blood disorders and certain cancers. Orthopedic applications using a patient’s own minimally manipulated cells (like BMAC) occupy a legal gray area that requires careful clinical judgment. We follow FDA regulations strictly and only offer procedures that are compliant with current standards.
From an evidence standpoint, results in clinical trials have been mixed. A landmark multicenter trial involving 480 patients found that MSC knee injections were no more effective than corticosteroid injections in terms of pain scores. Other trials, including those tracking autoimmune arthritis, show more promising results. Our position is that evidence is evolving and patient selection matters enormously. We do not present stem cell therapy as a guaranteed cure. We present it as a potentially beneficial option for carefully selected patients who understand the current state of research.
Financially, stem cell procedures typically cost between $3,000 and $8,000 for a single joint injection. Insurance generally does not cover these treatments given their investigational status. We discuss this upfront during consultations so patients can make fully informed decisions.
South Florida Multispecialty Medical Group offers something that standalone stem cell clinics cannot: a fully integrated multispecialty team. When a patient comes to us with arthritis, they benefit from the combined expertise of rheumatology, sports medicine, podiatry, and vascular surgery, all under one roof. For patients managing ankle arthritis treatment, this multispecialty model means the foot and ankle team works directly alongside our rheumatologists from day one.
After treating hundreds of patients with joint and autoimmune conditions in Miami, the single most important factor in positive outcomes is a thorough, individualized evaluation. We do not offer a one-size-fits-all injection protocol. We review your imaging, your labs, your treatment history, and your goals, and then we develop a treatment plan that makes clinical sense for you specifically.
Our regenerative medicine program includes stem cell therapy, PRP therapy, and Remy laser therapy as complementary modalities. Many patients benefit from a combination approach where, for example, a BMAC injection is followed by a structured course of physical therapy and laser therapy to maximize joint healing. We also coordinate closely with our rheumatology team to ensure that any ongoing pharmaceutical treatment (DMARDs, biologics) is optimized alongside regenerative interventions.
If you are in Miami or South Florida and considering stem cell therapy for arthritis, we invite you to schedule a consultation. We will give you a straight answer about whether you are a candidate, and if you are not, we will tell you that too, along with what we think will actually help.
Roughly 80 percent of strokes are preventable, yet carotid artery disease often gives no warning before a stroke strikes. That statistic alone should change how

A dull ache above the heel after a run. Morning stiffness in the back of the ankle that eases once you get moving around
