Most ankle sprains are not the same injury. Inversion sprains happen far more often, while eversion sprains are less common but may point to a more significant injury pattern because they affect the strong ligament complex on the inside of the ankle.
That difference matters in real life. Pain location, swelling pattern, ligament damage, stability loss and recovery planning can all shift depending on whether the foot rolled inward or outward. At South Florida Multispecialty Medical Group, we look closely at that mechanism because accurate diagnosis shapes the right treatment plan from day one.
Why the Direction of the Roll Matters
When people say they “rolled” an ankle, they usually mean the foot moved beyond its normal range and stretched or tore stabilizing ligaments. The direction of that roll tells us which ligament group likely took the force and which complications we need to rule out.
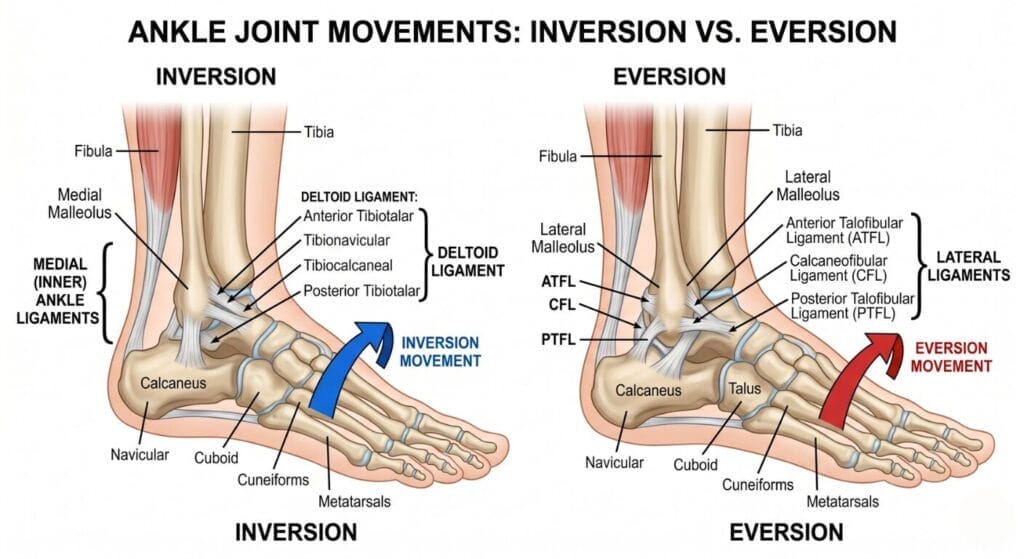
An inversion sprain means the foot turns inward and the ankle rolls outward, stressing the lateral ligaments on the outside of the ankle. An eversion sprain means the foot turns outward and stresses the deltoid ligament on the inside of the ankle.
That may sound like a small anatomical distinction, but it changes the injury story. Outer ankle injuries tend to be the familiar, classic sprains we see in sports and everyday missteps, while inner ankle injuries deserve extra attention because medial sprains are less common and often more severe.
What an Inversion Sprain Usually Looks Like
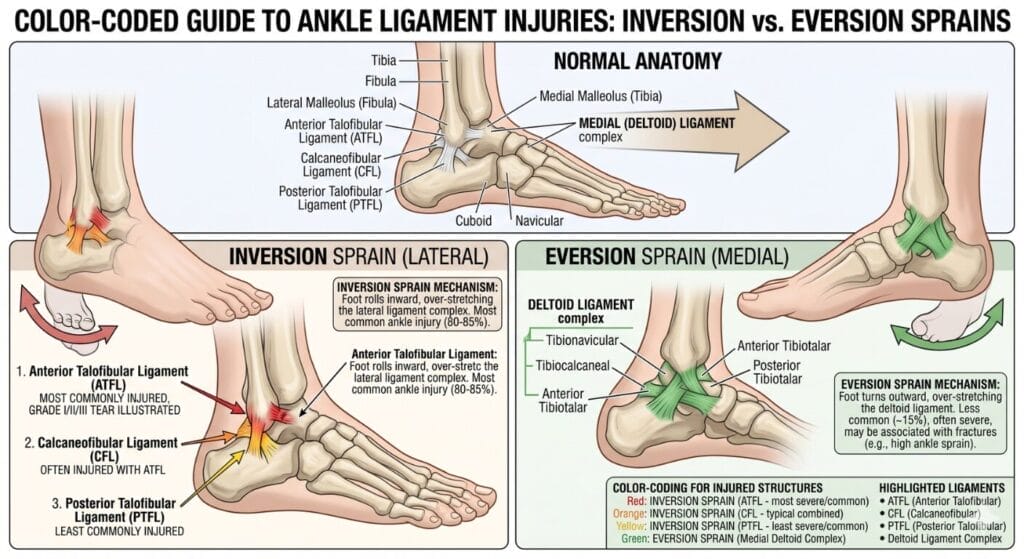
Inversion sprains are the ankle injuries most clinicians expect to see first because around 90% of ankle sprains involve an inversion mechanism. These injuries usually damage the lateral ligament complex, especially the anterior talofibular ligament and calcaneofibular ligament on the outer side of the ankle.
The typical story is familiar. Someone steps off a curb, lands on another player’s foot, cuts during pickleball, basketball or tennis, and the ankle folds inward fast enough to stretch or tear the outside ligaments.
Pain usually centers on the outer ankle in this pattern. Swelling, tenderness, bruising and a sense that the ankle feels weak or shaky are all common, and more severe tears can make weight bearing difficult.
In many mild cases, patients can still walk, although it is uncomfortable. Grade 1 and some Grade 2 sprains may allow walking with pain or mild instability, while complete tears are more likely to cause major swelling, bruising and trouble bearing weight.
What an Eversion Sprain Usually Looks Like
An eversion sprain happens when the foot rolls outward and away from the body, stretching the ligaments on the inside of the ankle. The main structure involved is the deltoid ligament, a strong and thick ligament complex that helps stabilize the medial side of the joint.
Because the deltoid ligament is stronger and thicker than the lateral ligaments, eversion sprains happen less often. When they do happen, they may be more severe and can create more concern about ankle instability or associated injury.
Patients with eversion sprains usually describe pain on the inner side of the ankle. They may also notice swelling, bruising, tenderness near the medial ankle and a sharper sense that pushing off or changing direction feels unsafe.
We often tell patients not to dismiss medial ankle pain as “just a twist.” An inner ankle sprain is less common than a lateral sprain, so it deserves a careful exam to confirm whether the injury is isolated or part of a broader ankle problem.
Ligaments Involved in Each Injury
The ankle relies on several ligament groups to stay stable as we walk, pivot and absorb force. On the outside, the major lateral ligaments include the anterior talofibular ligament, calcaneofibular ligament and posterior talofibular ligament.
In inversion sprains, the anterior talofibular ligament is commonly the first structure injured because it is especially vulnerable when the ankle rolls inward. Depending on severity, the calcaneofibular ligament and sometimes the posterior talofibular ligament can also be involved.
On the inside of the ankle, the deltoid ligament provides strong medial support. Eversion injuries stress this ligament, and that is one reason medial sprains are less common yet often taken seriously when they appear.
This anatomy also explains why pain location is such a useful clue during evaluation. Outside pain points us toward a lateral sprain, while inside pain raises suspicion for a deltoid ligament injury or another medial ankle issue that should not be overlooked.
How Symptoms Differ at First Glance
In both sprain types, patients can develop pain, swelling, bruising, stiffness and limited range of motion. The shared symptoms are why people often use the word “sprain” as if every ankle injury behaves the same, even though the damaged structures may be very different.
Still, a few patterns help separate them early. Inversion sprains usually hurt on the outside of the ankle, while eversion sprains usually hurt on the inside.
Inversion sprains are more common after sports cuts, jumps and awkward landings. Eversion sprains are less common, and when they happen clinicians stay alert because the injury mechanism can involve stronger forces or more substantial ligament disruption.
Severity matters just as much as sprain direction. A mild inversion sprain can be less disruptive than a severe eversion sprain, but a severe inversion sprain with complete tearing and instability can also be a major injury that needs structured care and rehabilitation.
Understanding Sprain Grades
Doctors do not classify ankle sprains only by direction. They also grade them by how much ligament damage occurred and how unstable the ankle becomes.
Grade 1: Mild stretching or slight tearing with mild pain and swelling, little to no bruising and no significant joint instability.
Grade 2: Partial tearing, more swelling, more pain, bruising and some loss of motion or stability.
Grade 3: Complete tearing of the ligament, severe swelling, pain, bruising and marked instability. Walking may be very difficult and the ankle may feel as if it will give way.
This grading framework applies to both inversion and eversion sprains. In practice, it helps us explain why one patient may recover in a couple of weeks while another needs bracing, therapy and a much longer return-to-activity timeline. Learn more about how we assess and treat all grades of ankle sprains at South Florida Multispecialty Medical Group.
When It May Not Be “Just” a Sprain
Not every rolled ankle is a straightforward ligament injury. Persistent inability to bear weight, worsening swelling, severe instability or pain that does not improve should prompt a professional assessment because fractures and other injuries can mimic or accompany sprains.
A high ankle sprain is another pattern clinicians consider. Unlike standard inversion or eversion sprains, a high ankle sprain affects the ligaments above the ankle that connect the tibia and fibula, and these injuries often take longer to recover from.
Imaging may become part of the workup when the exam suggests something more complex. Physicians may use X-rays for bones, MRI for ligaments and tendons, and CT scans for injuries that need more detailed three-dimensional imaging.
This is one reason we encourage patients not to self-diagnose based on swelling alone. Outer swelling may point toward a common lateral sprain, but inner ankle pain, major bruising, repeated giving way or severe weight-bearing pain deserve a closer look.
Treatment Basics for Both Sprain Types
Early care usually starts with rest, ice, compression and elevation. The RICE method is the backbone of initial ankle sprain care, especially in the first phase after injury.
That said, modern care does not stop at resting the joint. For many mild to moderate sprains, early guided movement is encouraged because it supports healing, circulation and a safer return of function.
Pain control may include anti-inflammatory medication when appropriate. Temporary bracing or a walking boot may also help protect the ankle, especially when swelling, pain or instability make normal walking difficult.
Most inversion and eversion sprains improve without surgery. Conservative care such as activity modification, bracing, physical therapy and progressive exercise is the standard path for most patients as long as the ankle regains stability and function over time.
How Treatment Emphasis Can Differ Between Inversion and Eversion Injuries
With inversion sprains, treatment often focuses on calming pain and swelling early, then rebuilding strength, balance and confidence in the lateral ankle. Because these sprains are so common, one of the biggest mistakes is returning to activity too soon and skipping the rehabilitation needed to restore stability.
With eversion sprains, the initial steps may look similar, but the threshold for careful reassessment is often lower because medial sprains are less common and may signal a more substantial injury pattern. If inner ankle pain is pronounced or the ankle remains unstable, further imaging or specialist follow-up may be needed.
In both cases, structured rehabilitation matters. Our sports medicine team in Miami helps restore range of motion, strength, agility and balance, and lowers the risk of another sprain by addressing the stability deficits that often linger after pain settles down.
Rehabilitation and Recovery Timeline
Recovery depends less on whether the word “sprain” sounds minor and more on grade, ligament damage and rehab quality. Grade 1 sprains may heal in about one to two weeks, Grade 2 injuries often take three to six weeks, and Grade 3 sprains can take weeks to months and sometimes need surgery when instability persists.
According to the Centers for Disease Control and Prevention (CDC), musculoskeletal injuries including ankle sprains are among the most common reasons for activity limitations in adults across the United States. Recovery for more complex injuries, including high ankle sprains, can take substantially longer than standard lateral sprains.
Rehab usually moves in stages. Early work restores motion and controls swelling, then strengthening and resistance exercises return, followed by balance drills, movement retraining and sport-specific progression when the ankle can tolerate load again.
We often compare ankle rehab to rebuilding trust after a fall. Pain may fade first, but balance, reaction speed and confidence usually recover later, and stopping rehab when the ankle “feels okay” is one reason recurrent sprains keep happening.
Long-Term Problems if Treatment Is Rushed
A poorly managed ankle sprain can create problems long after bruising fades. Untreated or recurrent injuries can lead to chronic instability, repeated sprains, lasting pain and early arthritis.
If ligaments tear completely and the ankle remains unstable, that instability can gradually damage bone and cartilage over time, according to the American Academy of Orthopaedic Surgeons (AAOS).
Past trauma is also one of the main drivers of ankle arthritis. Post-traumatic arthritis from prior ankle injuries, including repeated sprains, accounts for a large share of ankle arthritis cases. Our podiatry specialists in Miami are experienced in managing both acute sprains and the long-term complications that can follow when injuries are not properly treated.
This is why proper rehab is not optional for active adults, athletes or anyone whose job keeps them on their feet. A sprain that never fully regains stability often returns as another sprain, a chronic wobble or pain that starts showing up on stairs, uneven ground or long work shifts.
When to Seek Prompt Medical Care
You should seek medical attention if you cannot bear weight, swelling keeps worsening, pain remains significant after the first 48 hours or the ankle feels unstable. We also recommend evaluation for recurring injuries or symptoms that do not improve as expected.
Inner ankle pain deserves particular attention because medial sprains are less common. If the pain sits mainly on the inside of the ankle after an outward roll, an eversion injury should be considered and the joint should be examined carefully.
We also advise patients to get checked when they hear a pop, see major bruising spread quickly or suspect a fracture. An accurate diagnosis early on often shortens recovery because treatment becomes more precise from the start. Our foot and ankle care team provides thorough evaluations and personalized treatment plans for all types of ankle injuries.
How to Reduce the Chance of Another Sprain
Prevention starts with strength and balance. We recommend strengthening ankle and leg muscles, improving balance, wearing supportive shoes and considering bracing during high-risk activities to reduce re-injury risk.
After a first sprain, many athletes benefit from dedicated stability work rather than waiting for the ankle to “toughen up” on its own. Balance drills, resistance-band exercises and gradual return-to-sport progression help rebuild the control that protects the joint during sudden cuts, jumps and uneven steps.
Supportive footwear also matters more than many patients expect. Shoes that control motion and match the activity can reduce stress on a recovering ankle, especially during the weeks when tissues are healing but confidence and neuromuscular control have not fully returned. For a broader look at how foot biomechanics affect recovery, visit our comprehensive podiatry services page.
What Patients Should Remember
Inversion and eversion sprains are both ankle sprains, but they are not interchangeable diagnoses. Inversion injuries are far more common and affect the lateral ligaments on the outside of the ankle, while eversion injuries affect the stronger deltoid ligament on the inside and may be more serious when they occur.
The fastest way to make a sprain linger is to treat every ankle injury as routine. Knowing where the pain sits, how the ankle rolled, whether weight bearing is possible and how stable the joint feels helps guide the next step, from home care and bracing to imaging, therapy or specialist evaluation.
For patients in Miami who want a careful diagnosis and a recovery plan that protects long-term mobility, our podiatry and sports medicine teams at South Florida Multispecialty Medical Group evaluate ankle sprains with that bigger picture in mind. We aim to relieve pain, restore stability and help patients return to work, exercise and everyday movement with confidence.
Dr. Peter Hanna is a board-certified podiatrist and reconstructive foot & ankle surgeon with over 15 years of experience. He serves as Director of Podiatry at South Florida Multispecialty Medical Group, specializing in complex reconstruction, minimally invasive surgery, and diabetic foot care.