
Blog
Carotid Artery Disease: Symptoms & Treatment Options
Roughly 80 percent of strokes are preventable, yet carotid artery disease often gives no warning before a stroke strikes. That statistic alone should change how


Most people use “flat feet” and “fallen arches” as if they mean the same thing. Medically, they do not. We see this confusion all the time in our clinics at SFL Medical Group. It matters because treatment, expectations, and even surgery decisions can change once we sort out what is going on under each foot.
Think of your foot as a dynamic bridge. Arches give that bridge height and spring. Problems fall into two broad categories.
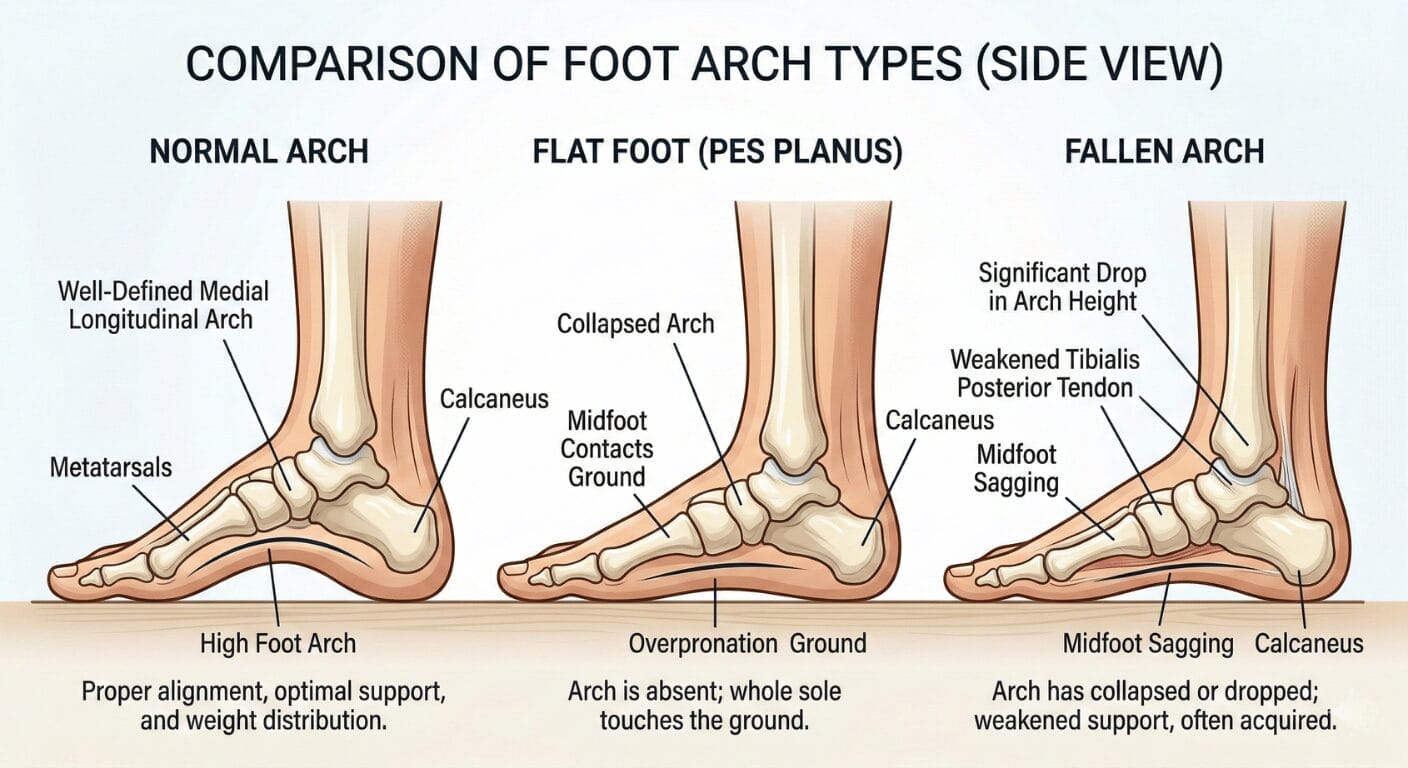
Flat feet mean you have little or no visible arch when you stand. This usually starts in childhood and often has a strong structural or genetic component.
Key points about flat feet:
We usually divide flat feet into two types.
The arch appears when you sit or stand on tiptoes but collapses under full weight. This is very common in kids and young adults. It is often painless but can predispose to overuse injuries if you are very active or gain weight.
The arch remains flat regardless of position. This can be due to bone deformities, tarsal coalitions, advanced arthritis, or old injuries. Rigid flat feet are more likely to cause pain and stiffness, and they need specialist evaluation.
Fallen arches describe arches that used to exist and have dropped over time. This is an acquired condition. The most common cause in adults is weakening of the posterior tibial tendon on the inside of the ankle. When that tendon weakens or tears, the arch slowly collapses. We call this posterior tibial tendon dysfunction (PTTD) or adult acquired flatfoot.
Key points about fallen arches:
The short version: flat feet are usually something you are born with or develop early. Fallen arches usually develop later because the structures that support the arch wear down or fail.

Even if you never thought about your arches at 30, you may notice real changes by 50, 60, or 70.
When arches flatten with age, ankles rotate inward, knees may drift inward, and hips and lower back absorb more rotational stress. We regularly see patients come in for knee or low back pain, and part of the solution ends up being better support under the arch.
Many people have lifelong flat feet and no pain at all. If flat feet do not hurt, restrict activity, or cause repeated injuries, we focus on monitoring and prevention rather than aggressive intervention.
Most young children have flexible flat feet. Arches often develop gradually until around age 8 to 10. Simply low arches in an active, pain free child rarely require rigid supports or surgery.
For adult acquired flatfoot, early intervention makes a huge difference. Bracing, targeted physical therapy, weight management, and shoe modifications can slow or even stop progression for many patients.
Minimalist shoes can strengthen feet in some people when introduced slowly. However, they can also overload a degenerating tendon or arthritic joint. For older adults with new arch pain, jumping into unsupportive footwear often worsens symptoms.
If you notice several of these, especially if one foot is clearly worse, we recommend an evaluation by a podiatrist or orthopedic foot and ankle specialist.
We ask about when symptoms started, occupational demands, shoe habits, previous injuries, and medical conditions like diabetes, rheumatoid arthritis, or obesity. On exam we look at foot shape in various positions, alignment of heel, ankle, knee, and hip, range of motion, tenderness along the posterior tibial tendon and plantar fascia, and muscle strength.
Imaging may include X rays for bone alignment and arthritis, ultrasound or MRI for tendon tears, and gait analysis to guide orthotic design.
Supportive footwear: We almost always start by optimizing shoes. Look for a firm heel counter, moderate arch support or removable insole, slight heel to toe drop, enough forefoot width, and a cushioned yet stable midsole.
Orthotics and bracing: Over the counter arch supports work well for mild, flexible flat feet. Custom orthotics are designed from your foot shape and pressure patterns. Ankle foot orthoses provide external support for more advanced cases.
Physical therapy: We prescribe strengthening for posterior tibial muscle, intrinsic foot muscles, and hip stabilizers. Stretching tight calf and Achilles muscles is equally important. Home exercises include calf stretches, heel raises, towel curls, and ankle inversion with resistance bands.
Injections and medications: NSAIDs for short term pain control, corticosteroid injections used cautiously for significant inflammation, and systemic medications from rheumatology to protect foot joints in conditions like rheumatoid arthritis.
Lifestyle changes: Every extra pound adds several pounds of force through each foot with every step. We coordinate with primary care and nutrition and encourage low impact exercise while getting feet under control.
Surgery is considered when conservative care has failed over several months, pain interferes with work, walking, or sleep, deformity continues to progress, or joints develop severe arthritis. Options may include tendon repair, tendon transfers, heel bone osteotomy, midfoot fusions, or procedures to correct bone shape.
At SFL Medical Group, we approach flat feet and fallen arches as part of your whole musculoskeletal system. Our collaborative approach includes podiatry and orthopedic evaluation, imaging and gait assessment, coordinated plans with physical therapists and primary care, and guidance on footwear, orthotics, and activity modification tailored to your daily life.
If you notice new arch changes, ankle pain, or progressive difficulty walking, this is the right time to be evaluated.
Roughly 80 percent of strokes are preventable, yet carotid artery disease often gives no warning before a stroke strikes. That statistic alone should change how

Nine out of every ten people diagnosed with lupus are women, and most receive their diagnosis between the ages of 15 and 44. That
